Original publication: garden state focus, Fall 2024, VOL. 72, NUM 1
New Jersey Chapter, Healthcare Financial Management Association
Younger HFMA members are largely unaware of New Jersey’s transformational role in America’s healthcare reform efforts. For about a 20-year period from 1974-1993, much of the fundamental work in developing inpatient prospective payment systems happened right here. This article briefly highlights those developments, beginning with Medicare and Medicaid enactment.
In 1965, Title XVIII – Medicare (named for Canada’s program of health care access for all) was enacted, assuring health care services for the elderly when they most need it, followed by Title XIX – Medicaid – enacted as a joint federal-state program to expand coverage for the working poor. In 1966, the country’s first Medicare hospital claim was processed by Blue Cross of New Jersey (now Horizon) and delivered to Jack Farmer, CFO of East Orange General Hospital. It made the five o’clock news.
Budget Review (1968-74)
The expansion of access to healthcare services was accompanied by rapidly rising costs, and New Jersey was no exception. Initially, the state relied on a voluntary budget review process where hospitals submitted their budgets to an advisory committee appointed by the Commissioner of Insurance. The advisory committee reviewed the budget submissions and recommended rate ceilings to Blue Cross. However, costs continued to escalate rapidly.
In 1971, Republican Governor William Cahill signed the Health Care Facilities Planning Act, , N.J. Stat. Ann. §§ 26:2H-1 to 26:2H-26, establishing a Certificate of Need planning process and authorizing the state Departments of Health and Insurance to jointly set inpatient Blue Cross and Medicaid payment rates. It also mandated participation of all hospitals in a budget review program.
Following enactment, the state delegated the budget review process to the Hospital Research and Education Trust, a subsidiary of the New Jersey Hospital Association. HRET reviewed the budgets and recommended per diem rate ceilings for Blue Cross and Medicaid. Two years in, the New Jersey Public Interest Research Group issued a blistering report, “Bureaucratic Malpractice,” describing HRET’s process as “the fox guarding the chicken coop,” and the state was directed to take over the rate-setting process.
Per-Diem Rates (1975-79)
Newly-elected Democratic Governor Brendan Byrne’s cabinet included James Sheeran as Insurance Commissioner and Dr. Joanne Finley as Commissioner of Health. Sheeran had been Byrne’s high school classmate, mayor of West Orange and chair of “Republicans for Byrne.” He also was a decorated World War II veteran and a consumer advocate. Joanne Finley had been serving as Director of Public Health in New Haven at the time she was appointed to the Byrne cabinet. Previously, Dr. Finley was Vice President for Medical Affairs with Blue Cross of Philadelphia and headed health planning in that city from 1968 to 1972.
Both commissioners saw eye-to-eye and, following the blistering NJPIRG report, took on the hospital rate setting challenge. The state issued a request-for-proposals for a contractor to develop and implement an inpatient hospital rate-setting system. Given their experience in doing so for the state of Maryland, Haskins & Sells (now Deloitte) was selected to develop 1975 inpatient rates for New Jersey’s hospitals. John Dalton was assigned as Project Manager to get it done, reporting to Sister Cathleen Maloney, SC, CPA, Chief of the Rate Setting Program.
Sister Cathleen was the first member of her order to become a CPA and was Controller at St. Elizabeth’s Hospital before joining the Department of Health. She reported to Assistant Commissioner John B. Reiss, who had been a Health Economics Professor at Stockton State College before joining the Department.
The consulting contract was finalized in early September and, in a fast and furious four months, the project team:
- Recruited and trained seven rate analysts (Gene Arnone, Mike Dively and Jim Hull; then Joe Lario, Chuck Lydon, George Popko and Al Rabin).
- Designed cost-reporting worksheets for the Standard Hospital Accounting and Rate Evaluation System (SHARE) that hospitals would use to report functional costs for about 30 cost centers.
- Developed a classification system for peer groups of hospitals by type (major teaching, minor teaching and nonteaching community hospital) and location (inner city, urban, suburban and rural). At the time, New Jersey had one county classified as rural – Hunterdon. Specialized and rehabilitation hospitals continued to be subject to budget review.
- Promulgated regulations describing the rate-setting process, and included an appeal option for providers dissatisfied with their Blue Cross and Medicaid prospective pre diem payment rates. The regulations were challenged by NJHA as violating the Administrative Procedures Act’s comment period requirements, but compliance with the APA would have left hospitals without updated payment rates well into 1975.
- Worked with NJHA and NJHFMA to recruit a panel of hospital CFOs to advise on reclassification recommendations from responsibility accounting to functional reporting. They included Jim Carroll from Morristown Memorial Hospital, Tom Dalton from Overlook Hospital, Jack Farmer from Hackensack Hospital and Keith McLaughlin from Perth Amboy General Hospital.
- Wrote and issued a twice-monthly “Health & Insurance Newsletter” to update hospitals on progress.
- Conducted on-site briefings and training sessions in each of the state’s four regional planning districts.
By late November, reports began flowing in from hospitals. They were desk-checked by the rate analysts for accuracy and completeness, then either sent back to the hospital for corrections or passed on to data entry. System testing began in earnest, and the rate analysts were able to begin reviewing results and verifying per diem inpatient payment rates for their assigned hospitals.
By mid-January 1975, inpatient per diem payment rates were set for New Jersey’s 108 acute care hospitals. It came as no surprise that most of the hospitals were not pleased with the results. Most hospitals appealed their initial rate determination, arguing that the system did not adequately reflect the uniqueness of their service area and patient mix. NJHA advocated for changes to improve the system’s fairness. A number of changes were made to the SHARE regulations for 1976, and the Department of Health began to consider other approaches to rate setting.
All-Payor DRGs (1980-89)
As New Haven’s Director of Public Health, Dr. Finley had become familiar with work being done at Yale University to use clinical data about a patient’s condition to predict how long a patient would stay in the hospital. She recognized that this approach to utilization management might also provide a basis for rate setting. Professors John Devereaux Thompson and Robert Fetter were invited to make a presentation of their work at the Department of Health. I was at the presentation and still vividly recall Thompson stating, “If General Motors can cost out cars, hospitals can cost out patients.” Having recently completed design of a cost accounting system for a major textile manufacturer, Thompson’s statement made sense to me.
Commissioner Finley agreed that a patient-centric approach to rate-setting on a per case basis had the potential to be fairer than costs per diem that did not adequately reflect a hospital service area’s epidemiology and patient case mix. New Jersey then applied for a Medicare Sec. 1115 waiver for a demonstration project to implement an inpatient payment system for all payors based on Diagnosis-Related Groupings (DRGs).
In 1976, Michael Kalison was retained to head up the demonstration project. A recent graduate of the Law School at the University of Pennsylvania, he had served a clerkship with the New Jersey Supreme Court. In early 1977, Jo Surpin joined as a case-mix analyst and later as Assistant Project Manager. With a $4 million dollar grant, the Medicare waiver and enabling legislation (Chapter 83, which also established the Hospital Rate Setting Commission to set and adjust the schedule of reimbursement rates used by New Jersey hospitals), New Jersey designed and implemented the country’s first prospective payment system where payment per inpatient case was based on illness primarily as defined by specific ICD-9 diagnosis and procedure codes.
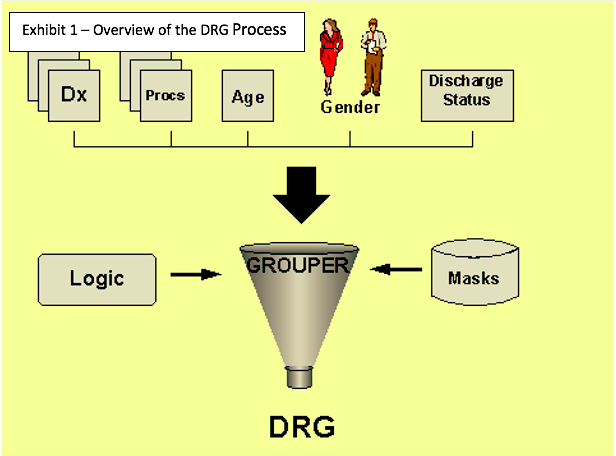
Clinical information was merged with other information, including patient demographic data, to be “grouped” into the applicable DRGs (see Exhibit 1). Initially, there were 383 DRGs in 25 major diagnostic categories.
Hospitals had advocated for inclusion of all uncompensated care in the prospective payment rates, both charity care (can’t pay) and bad debt (won’t pay). Their insistence on inclusion of bad debt ultimately proved to be a fatal error.
Joe Morris had joined the Department of Health as a rate analyst in 1977, and when Mike Kalison left, replaced him as Project Manager in March 1979, nine months before the first group of hospitals transitioned from SHARE to DRGs. Dr. Bruce C. Vladeck had succeeded John Reiss as Assistant Commissioner of Health. Vladeck subsequently served as Administrator of the Health Care Financing Administration (now CMS) from May 1993 to September 1997.
Over a three-year period (1980-82), New Jersey’s acute care hospitals transitioned from SHARE to DRGS:
- 26 hospitals pioneered the transition in 1980;
- 36 hospitals joined in 1981, bringing the total to 62;
- 1982 – All 96 hospitals were phased into DRGs.
At the federal level in 1982, the Tax Equity and Fiscal Responsibility Act (TEFRA) modified the Section 223 Medicare hospital reimbursement limits to include a case mix adjustment based on DRGs. In 1983 Congress amended the Social Security Act to include a national DRG-based Prospective Payment System for all Medicare patients (2). The pioneering efforts of the New Jersey demonstration project were being adopted nationally.
The Medicare waiver would continue in effect so long as the Medicare program spent less than it would have under its new Prospective Payment System. Although payment per case incentivized hospitals to focus on reducing length of stay, inclusion of bad debt as an element of allowable cost eventually led to New Jersey’s costs exceeding what Medicare would have paid and the 1989 loss of the Medicare waiver.
All but Medicare DRGs (1989-93)
New Jersey attempted to continue with an “all but Medicare” DRG system, adding a state-mandated surcharge to cover uncompensated care, Medicare shortfall and prior years’ payment shortfalls. In 1990, the United Wire, Metal & Machine Health & Welfare Fund filed suit against 14 New Jersey hospitals contending that they need only pay the actual charges on inpatient hospital bills, exclusive of state-mandated surcharges and markups (3).
A total of 14 unions “piggy backed” on the original suit and 70 hospitals were named as defendants along with the state and the Commissioner of Health. They argued that, as self-insured employer funds protected by the Employee Retirement and Income Security Act of 1974 (ERISA), they were exempt from paying surcharges that result from state regulations. They contended that mark-ups such as adjustments for uncompensated care, Medicare shortfalls and other cost shifts represented hidden and illegal taxes.
When District Court Judge Alfred M. Wolin ruled for the plaintiffs, the May 28, 1992, banner headline in the Star-Ledger read, “Judge derails hospital rate system.” The decision in favor of the ERISA plans was appealed.
However, given the uncertainty of the appeal’s likelihood of success and concerns about the imminent expiration of the Health Care Trust Fund, the legislature enacted the Health Care Reform Act of 1992 (HCRA-92) that, among other actions,
- Diverted $1.6 billion, over three years, from the Unemployment Insurance Fund to finance charity care;
- Expanded charity care eligibility criteria and provided that charity care be paid at Medicaid rates;
- Continued the Hospital Rate Setting Commission for a one-year transition to a deregulated system;
- Eliminated DRG billing for non-federal payors and enabled hospitals to bill charges; and
- Imposed a cap on hospital revenues for 1993.
The last-minute addition of the revenue cap provision placed many hospitals in a threatening financial condition rather than having one final year (1993) to recover prior years’ undercollections. Nonetheless, 1993 marked the dawn of deregulation for New Jersey’s hospitals.
In an ironic footnote, the Third Circuit Court reversed Judge Wolin’s decision in April 1993. The 2-1 ruling supported the position taken by the Department of Health and the New Jersey Hospital Association that ERISA did not preempt the Chapter 83 rate-setting system. The appeals court found that New Jersey’s rate-setting system was not intended to regulate the affairs of ERISA plans. Rather, the uncompensated care add-ons, Medicare shortfalls and discounts to certain payers were all part of doing business.
Frank Ciesla, who argued the case for NJHA, stated “While this is clearly a win, no new ground was broken with this decision. If you’re looking for new insight into ERISA applicability, you won’t find it here.” Unfortunately, the decision came too late as the sun already had set on New Jersey’s innovative experiment that became the template for Medicare’s Inpatient Prospective Payment System, still in use today.
Dr. Finley’s Vision Transformed Hospital Care
Ten years ago, an article in the Annals of Internal Medicine took a retrospective look at 30 years of DRGs. Author Kevin Quinn argued that Medicare paying hospitals by diagnosis-related group was “the most influential innovation in the history of health care financing” (4). Quinn stated that “The strong incentives were revolutionary in their impact.” The change from cost reimbursement to prospective payment incentivized hospitals to become more cost-effective. His literature survey concluded that none of the worst fears about adverse effects on patients were realized.
And it all began right here in the Garden State.
References:
- Hospital Rate Setting and Patient Access Under the New Jersey Hospital Rate Setting System, by Glenn Melnick, Joyce Mann and Carl Serrato, the RAND Corporation, September 1988
- Design and development of the Diagnosis Related Group (DRG), Centers for Medicare and Medicaid Services, PBL-038, October 2019
- United Wire, Metal & Mach. Health & Welfare Fund v. Morristown Memorial Hosp., 995 F.2d 1179, 1993
- After the revolution: DRGs at age 30, by Kevin Quinn, Annals of Internal Medicine, March 2014

John J. Dalton, FHFMA serves as Senior Advisor Emeritus at BESLER and Editor of the Three Minute ReadTM, the twice-monthly newsletter of the Healing American Healthcare Coalition. A Past President of the New Jersey Chapter and National Board member, he was the 2001 recipient of the Frederick C. Morgan Award for Individual Lifetime Achievement. The New Jersey Hospital Association named him as its 2017 Hospital Trustee of the Year.
